Chondromalacia of the Patella (Runners Knee, Patellofemoral Pain)
Description:
The knee is a complex joint. It includes the articulation between the tibia and femur (leg and thigh) and the patella (knee cap). The most common knee problems in running relate to what is called the "patellofemoral complex". This consists of the quadriceps, knee cap and patellar tendon. What is now called
Chondromalacia of the patella, or Patellar Femoral Pain Syndrome (PFPS) as well
as runner's knee.
Cartilage does not have the same blood supply that bone does. It relies on intermittent compression to squeeze out waste products and then allow nutrients to enter the cartilage from the synovial fluid of the joint. During running certain mechanical conditions may predispose you to a mistracking knee cap. Portions of the cartilage may then be under either too much or too little pressure and the appropriate intermittent compression that is needed for waste removal and nutrition supply may not be present. This may result in cartilage deterioration, which at the knee usually occurs on the medial aspect or inner part of the knee cap. All patello-femoral pain though may not be caused by this mechanism, although uneven stresses across the joint are believed to play an important role in the development of pain in this area.
the knee.
Anatomy
The symptoms of runners knee include pain near the knee cap usually at the medial (inner) portion and below it. Pain is usually also felt after sitting for a long period of time with the knees bent. Running downhill and sometimes even walking down stairs can be followed by pain. This has been called the "movie theatre sign". Patellofemoral pain syndrome is often caused by the kneecap not tracking smoothly in its femoral groove. The symptoms are aggravated when the knee is bent since (with increased vectors of force) increased pressure exists between the joint surface of the knee cap and the articular surface of the femur (thigh bone). This increase in force over-stresses the injured area and leads to pain.
Causes:
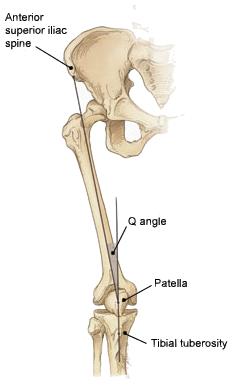
Factors that increase what is known as the "Q" (Quadriceps) angle increases the chance of having runners knee. The Q angle is an estimate of the effective angle at which the quadriceps averages its pull. It is determined by drawing a line from the Anterior Superior Iliac Spine (bump above and in front of your hip joint) to the center of your knee cap and a second line from the center of your knee cap to the insertion of the patellar tendon (where the tendon below your knee cap inserts). Normal is below 12 degrees, abnormal is usually considered to be above 15 degrees. Many times adding to the strong lateral pull of the bulk of the quadriceps is a weak vastus medialis. This is the portion of the quadriceps that helps medially stabilize the patella. It runs along the inside portion of the thigh bone to join at the knee cap with the other three muscles making up the quadriceps. Some of the mechanical conditions that may contribute to this include:
| Wide Hips (female runners) Knock Knees (Genu Valgum) Subluxating Patella Patella Alta (high patella) Small medial pole of patella or corresponding portion of femur Weak Vastus Medialis Weak Quadriceps Muscles Tight Hamstrings or calf muscles Pronation of the feet |
The "Q" angle |
Treatment of Chondromalacia of the Patella
At an early stage running should be decreased to lessen stress to this area and allow healing to begin. It is important to avoid downhill running which stresses the patello-femoral complex.
Exercises performed with the knee bent should be avoided. When the knee is bent the forces under the knee cap are increased. Many people feel that the vastus medialis muscle works only during the final thirty degrees of extension of the knee. This is the muscle that helps stabilize the knee cap medially and prevents it from shifting laterally and tracking improperly at the patello-femoral joint. The Vastus Medialis Oblique
and Vastus Medialis Longus have been shown to be considerably weaker than the Vastus Lateralis
in patients with Patellofemoral Pain Syndrome compared to normals. Straight leg lifts strengthen the vastus medialis muscles and do not significantly stress the undersurface of the knee cap.
consult your orthopedist, physical therapist or trainer for the correct
stretching techniques.
Tight posterior muscles should be stretched. In many cases tight calf muscles or hamstrings lead to a "functional equinous" and make the foot pronate while running or walking. This pronation is accompanied by an internal rotation of the leg which increases the Q angle and contributes to the lateral subluxation of the knee cap. On occasion a tight iliotibial band may contribute to
chondromalacia of the patella
If you over-pronate make sure you use shoes that offer more anti-pronation features. Move up a ranking in the amount of stability and pronation control that your shoes offer. If further control of pronation is needed orthotics should be considered.
Orthotics:
Orthotics can be a great assist in the therapy of patellofemoral pain syndrome and patellofemoral dysfunction. A variety of studies over the years have shown their effectiveness in treating this in
runners. Orthotics limit the maximum amount of excessive pronation. They also have been demonstrated to reduce the speed (acceleration) of internal tibial rotation. Reducing the speed of internal tibial rotation will reduce the amount of sudden stresses applied to the undersurface of the patella and the need for
the vastus medialis to work so hard in maintaining proper tracking and positioning of the patella. As per Newton's Laws slower motions will require less force to counterbalance them.