
Avascular Necrosis (Osteonecrosis, Osteochondritis) and the Foot and Ankle
Synopsis and Causes
Osteonecrosis is a disease resulting from the temporary or permanent loss of blood supply to the bones. Without blood, the bone tissue dies, and ultimately the bone may collapse. If the process involves the bones near a joint, it often leads to collapse of the joint surface. Osteonecrosis is also known as avascular necrosis, aseptic necrosis, and ischemic necrosis.
Avascular necrosis of the Navicular Bone
Although it can happen in any bone, osteonecrosis most commonly affects the ends (epiphysis) of the femur, the bone extending from the knee joint to the hip joint. Other common sites include the upper arm bone, knees, shoulders, and ankles.(discussed below) The disease may affect just one bone, more than one bone at the same time, or more than one bone at different times. According to the American Academy of Orthopaedic Surgeons, 10,000 to 20,000 people develop osteonecrosis each year, and most of them are between 20 and 50 years of age. Osteonecrosis is the underlying diagnosis in approximately 10 percent of hip replacements. Orthopaedists – doctors who specialize in the diagnosis and treatment of injuries and diseases of the musculoskeletal system – most often diagnose this disease.
The amount of disability that results from osteonecrosis depends on what part of the bone is affected, how large an area is involved, and how effectively the bone rebuilds itself. Normally, bone continuously breaks down and rebuilds – old bone is replaced with new bone. This process – which takes place after an injury as well as during normal growth – keeps the skeleton strong and helps it to maintain a balance of minerals. In the course of osteonecrosis, however, the healing process is usually ineffective and the bone tissues break down faster than the body can repair them. If left untreated, the disease progresses, the bone collapses, and the joint surface breaks down, leading to pain and arthritis.
Osteonecrosis is caused by impaired blood supply to the bone, but it is not always clear what causes that impairment. Osteonecrosis often occurs in people with certain risk factors (such as high-dose corticosteroid use and excessive alcohol intake) and medical conditions. However, it also affects people with no health problems and for no known reason. Following are some potential causes of osteonecrosis and other health conditions associated with its development.
Steroid Medications
Aside from injury, one of the most common causes of osteonecrosis is the use of corticosteroid medications such as prednisone. Corticosteroids are commonly used to treat inflammatory diseases such as systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowl disease, severe asthma, and vasculitis. Studies suggest that long-term use of oral or intravenous (IV) corticosteroids is associated with nontraumatic osteonecrosis. Patients should discuss concerns about steroid use with their doctor.
Doctors are not sure exactly why the use of corticosteroids sometimes leads to osteonecrosis. They speculate that the drugs may interfere with the body’s ability to break down fatty substances called lipids. These substances then build up in and clog the blood vessels, causing them to narrow and to reduce the amount of blood that gets to the bone. Some studies suggest that corticosteroid-related osteonecrosis is more severe and more likely to affect both hips (when occurring in the hip) than osteonecrosis resulting from other causes.
Alcohol Use
Excessive alcohol use is another common cause of osteonecrosis. People who drink alcohol in excess can develop fatty substances that may block blood vessels, causing a decreased blood supply to the bones.
Injury
When a fracture, a dislocation, or some other joint injury occurs, the blood vessels may be damaged. This can interfere with the blood circulation to the bone and lead to trauma-related osteonecrosis. In fact, studies suggest that hip dislocation and hip fractures are major risk factors for osteonecrosis.
Increased pressure within the bone may be another cause of osteonecrosis. When there is too much pressure within the bone, the blood vessels narrow, making it hard for them to deliver enough blood to the bone cells. The cause of increased pressure is not fully understood.
Other Risk Factors
Other risk factors for osteonecrosis include radiation therapy, chemotherapy, and organ transplantation (particularly kidney transplantation). Osteonecrosis is also associated with a number of medical conditions, including cancer, lupus, blood disorders such as sickle cell disease, HIV infection, Gaucher’s disease, Caisson disease, gout, vasculitis, osteoarthritis, and osteoporosis.
Who Is Likely to Develop Osteonecrosis?
Osteonecrosis affects both men and women. It can occur in people of any age, from children to the elderly. However, it is most common in people in their thirties, forties, and fifties.
In the Foot and Ankle
Freiberg's infraction
Due to the collapsed appearance, Freiberg originally termed the process an infraction of the second metatarsal head, therefore, it is now often termed Freiberg's infraction. It is now known that the process is that of true osteonecrosis resulting in collapse. While the second metacarpal head is the most common, involvement of the third is not uncommon.
The demographics of Freiberg's disease is quite distinct. It is much more commonly observed in females than males, approximately 3-4:1. The average age range seen is 13-18 years of age and is most commonly unilateral .
The cause of Freiberg's infraction is trauma, either acute or chronic. It is thought that the second metatarsal is most commonly involved because of its relative length and fixation as compared to the rest of the metatarsals. High heels, most commonly worn by females combined with the microtrauma that they cause to the heads of the metacarpals is often is blamed for the onset of Freiberg's disease.
Clinically, as with other forms of osteonecrosis, local pain, swelling, and redness are typical. Restriction of motion at the involved joint is also seen. The symptoms may start out as mild, but may progress to a chronic debilatating state eventually.
If you see one Freiberg's infraction, you've seen them all, as they say. The radiographic signs are very consistent and typical as seen below.
|
Freiberg's of the second metatarsal |
 Freiberg's |
The radiographic signs of Freiberg's infraction seen here include increased sclerosis, fragmentation and collapse/flattening of the second metatarsal. Other signs specific for this location include widening of the metatarsal head and widening and cortical thickening of the metatarsal shaft.
|
Freiberg's of the third metatarsal
|
Figure 3 illustrates AP and medial oblique views of a foot revealing Freiberg's disease of the head of the third metatarsal head with very similar radiographic changes as described in figures one and two.
Treatment is difficult. Some treatment regimes may include a felt donut cushion to ease pressure off the metatarsal head, ice to reduce pain and swelling, and ultrasound if there is no fragmentation. Properly fitted new shoes may be suggested if there is a history of routine use of high heel shoes.
Iselin's disease
Iselin's disease (traction apophysitis of the tuberosity(base) of the fifth metatarsal) has been reported rarely, but is probably more common than appreciated. It appears to be more common in athletically active older children and adolescents. most children spontaneously outgrow this condition
Koehler's Disease
Koehler's disease was thought by many to be avascular necrosis of the tarsal navicular primarily based on the radiographic signs. It is now a much more controversial subject. Kohler's disease is can be a very confusing and ambiguous entity due to uncertain etiology and often times vague symptoms. A history of trauma is only elicited in approximately 35% of cases and symptoms that correlate with the radiographic signs are very sporadic.
When a diagnosis of Kohler's disease is made, the typical patient is a young male, typically between 3 and 7 years of age. It is unilateral approximately 75% of cases.
The controversy of Kohler's disease stems from the fact that many authorities feel that this process is not a "disease" at all, but rather a process of altered, but completely normal, ossification of the tarsal navicular which leads to the radiographic appearance.
There are two main reasons for the idea that this often times is not osteonecrosis is the fact that 1) there are a lack of symptoms and 2) it is a self-limiting condition.
The radiographic appearance is sclerosis, overall flattening and deformity of the navicular. But, again, it's the associated signs and symptoms, as described that must be present for a confident diagnosis. MRI or bone scan may help confirm the diagnosis, but because of its self-limiting nature, it most likely is not warranted.
 |
 |
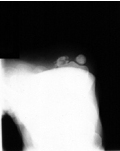
Sesamoidial Avascular Necrosis
Avascular necrosis of the sesamoids do not have an eponym to memorize, thank goodness. This condition is most present in active individuals commonly involved with dancing or running. Symptoms consist of focal pain, swelling and restricted range of motion. When it becomes revascularized, normal function and resolution of symptoms are expected.
 |
 |
Osgood-Schlatter disease
Osgood-Schlatter disease occurs in the tibial tubercle apophysis at the insertion of the patellar tendon. It occurs between the ages of 10 to 15, more commonly in boys. It is probably a form of overuse syndrome, due to repeated avulsion stress on the tibial tubercle. X-rays are usually normal, and the diagnosis is usually made clinically by localized tenderness over the tibial tubercle. Treatment consists of rest for a few days and use of non-steroidal anti-inflammatory medication. An Osgood-Shlatter brace to protect the patellar tendon and tibial tubercle may be used for sports. There is usually no need to restrict activities, as long as the child can tolerate the pain. No long term disability is expected, although there have been reports of cases where the tibial tubercle stays prominent and even tender long after maturation.
Symptoms, Diagnosis and Treatment
In the early stages of osteonecrosis, people may not have any symptoms. As the disease progresses, however, most experience joint pain. At first, the pain occurs only when putting weight on the affected joint. Later, it occurs even when resting. Pain usually develops gradually, and may be mild or severe. If osteonecrosis progresses and the bone and surrounding joint surface collapse, pain may develop or increase dramatically. Pain may be severe enough to limit range of motion in the affected joint. In some cases, particularly those involving the hip, disabling osteoarthritis may develop. The period of time between the first symptoms and loss of joint function is different for each person, but it typically ranges from several months to more than a year.
After performing a complete physical examination and asking about the patient’s medical history, the doctor may use one or more bone imaging techniques to diagnose osteonecrosis. As with many other diseases, early diagnosis increases the chances of treatment success. The tests described below may be used to determine the amount of bone affected and how far the disease has progressed.
X Ray
A radiograph, or x ray, is probably the first test the doctor will recommend. A simple way to produce pictures of bones, an x ray is often useful in diagnosing the cause of joint pain. For osteonecrosis, however, x rays are not sensitive enough to detect bone changes in the early stages of the disease. So if the x ray is normal, the doctor may order more tests. In later stages of osteonecrosis, x rays may show bone damage, and once the diagnosis is made, they are often used to monitor disease progression.
Magnetic Resonance Imaging (MRI)
Research studies have shown that magnetic resonance imaging, or MRI, is the most sensitive method for diagnosing osteonecrosis in the early stages. Unlike x rays, bone scans, and CT (computed/computerized tomography) scans (see below), MRI detects chemical changes in the bone marrow. MRI provides the doctor with a picture of the affected area and the bone-rebuilding process. In addition, MRI may show diseased areas that are not yet causing any symptoms. Some doctors caution against aggressive treatment of osteonecrosis that has been detected by MRI but is not causing symptoms. One study has shown evidence that for a select group of patients in the early stages of osteonecrosis, the disease may improve spontaneously.
Computed/Computerized Tomography (CT scan)
A CT scan is an imaging technique that provides the doctor with a three-dimensional picture of the bone. It also shows “slices” of the bone, making the picture much clearer than x rays and bone scans. Some doctors disagree about the usefulness of this test to diagnose osteonecrosis. Although a diagnosis usually can be made without a CT scan, the technique may be useful in determining the extent of bone damage. CT scans are less sensitive than MRIs.
Bone Scan
A type of test called technetium-99m bone scanning is used most commonly in patients who have normal x rays and no risk factors for osteonecrosis. In this test, a harmless radioactive material is injected through an intravenous line, and a picture of the bone is taken with a special camera. The picture shows how the injected material travels through blood vessels in bone. A single bone scan finds all areas in the body that are affected, thus reducing the need to expose the patient to more radiation.
Biopsy
A biopsy is a surgical procedure in which a tissue sample from the affected bone is removed and studied. Although a biopsy is a conclusive way to diagnose osteonecrosis, it is rarely used because it requires surgery.
Functional Evaluation of Bone
Tests to measure the pressure inside a bone may be used when the doctor strongly suspects that a patient has osteonecrosis, despite normal results of x rays, bone scans, and MRIs. These tests are very sensitive for detecting increased pressure within the bone, but they require surgery.
Appropriate treatment for osteonecrosis is necessary to keep joints from breaking down. Without treatment, most people with the disease will experience severe pain and limitation in movement within 2 years. To determine the most appropriate treatment, the doctor considers the following:
the age of the patient
the stage of the disease (early or late)
the location and whether bone is affected over a small or large area
the underlying cause of osteonecrosis. With an ongoing cause such as corticosteroid or alcohol use, treatment may not work unless use of the substance is stopped.
The goal in treating osteonecrosis is to improve the patient’s use of the affected joint, stop further damage to the bone, and ensure bone and joint survival. To reach these goals, the doctor may use one or more of the following surgical or nonsurgical treatments.
Nonsurgical Treatments
Usually, doctors will begin with nonsurgical treatments, alone or in combination. Unfortunately, although these treatments may relieve pain or help in the short term, for most people they don’t bring lasting improvement.
Surgical Treatment
A number of different surgical procedures are used to treat osteonecrosis. Most people with osteonecrosis will eventually need surgery.
For most people with osteonecrosis, treatment is an ongoing process. Depending upon the stage of the disease, doctors may first recommend the least complex or nonoperative treatment plans, such as medication or reduced weightbearing. If these modalities are unsuccessful, surgical treatments may be needed. It is important that patients carefully follow instructions about activity limitations and work closely with their doctors to ensure that appropriate treatments are used.
Prognosis
With proper treatment, most people with osteonecrosis can lead productive lives. But there is still a lot to learn about prevention, diagnosis, and treatment. Some goals of current research are to:

