Flexor Hallucis Longus Tendonitis
Anatomy & Function
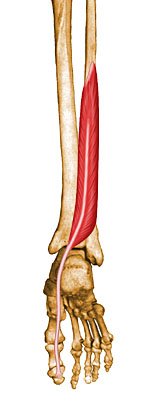
The flexor hallucis longus (FHL) tendon is one of three structures that lie in the tarsal tunnel. Running behind the medial malleolus (inside ankle bone), the FHL is the most posterolateral (to the rear and side). The FHL runs forward into the foot to insert onto the distal phalanx (the end bone) of the great toe. The FHL acts as a flexor of the great toe, elevates the arch, and assists with plantar flexion of the ankle (pointing the toes away from the body).
Location of the Flexor Hallucis Longus
Diagnosis And Treatment
Patients with FHL Tendonitis usually
present with pain in the posteromedial aspect of the ankle (behind the inside
ankle bone). The pain improves with rest and increases in sports requiring
push-off and extended running. Usually no palpable tenderness is present due to
the deep location of the tendon. Pain and weakness are noted with resistance to
plantar flexion of the first MTP joint. Pain also may be present in the tarsal
tunnel (the area just back of the inside ankle bone).
FHL tendonitis typically is associated with repeated push-off maneuvers, such as
those executed by ballet dancers or sprinters. Sometimes blunt trauma and
repetitive impact may also play a role. FHL tendonitis may occur at three sites.
These are: the entrance of the fibro-osseous tunnel between medial and lateral
talar tubercles (the prominent ankle bones on then inside and the outside part
of the ankle); the flexor sheath behind medial malleolus (inside ankle bone);
between the sesamoids (small bones) of the great toe.
Among the conditions that can look
like this are: Achilles tendinitis, Posterior Tibial Tendonitis, and tarsal
tunnel syndrome.
Clinical findings include: swelling, pain, and tenderness posterior to the
medial malleolus; triggering and pain along tendon sheath that may occur with
toe flexion (bending the toe down); and reduced ability to point the great toe
up. Plain x-rays of the foot are helpful with the differential diagnosis, and US
imaging or MRI can help rule out a tear.
Treatment consists of immobilization, activity restrictions, and NSAIDs. Orthotics may be used as a conservative measure - steroid injection is possible but caution must be exhibited because of the nerves and blood vessels in the area. in severe cases surgery is sometimes required.