| Bony
Structures of the Lower Leg, Ankle and Foot |
|
|
The foot contains 26
bones, 31 joints, and 20 intrinsic muscles (small muscles in the foot).
|
| The foot
and ankle are generally discussed by breaking them into several
anatomical regions. The ankle joint, which is the distal aspect of the
tibia and the fibula articulating with the talus, is the most proximal
joint. The foot is divided into the rearfoot, the midfoot and the
forefoot structures. |

|
| Distal
Tibia and Fibula |
|
|
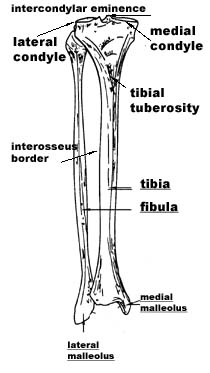
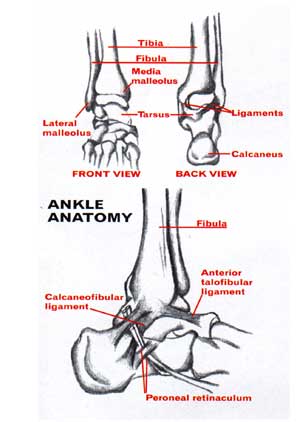
The proximal ends of
the tibia and fibula were discussed in Unit VII. The distal ends of
these two bones form the cornerstones of the ankle joint. The distal
tibia has a medial malleolus that forms the interior bump you feel on
the inner surface of the ankle. The distal fibula has a longer more
pointed bony structure called the lateral malleolus and is the bump you
can feel on the exterior surface of the ankle. Both of these bones have
articular surfaces that articulate with the talus to form the mortise
joint of the ankle. When
these two bones are in anatomical alignment they form a mostly square
joint space at their distal aspects. The body of the talus fits nicely
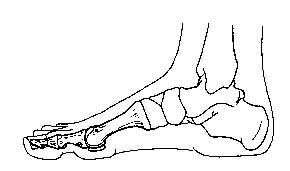
into this joint space. (Note the square space at the distal end of
the bones in the picture to the left. It is the space between the medial
and lateral malleoli) |
| The
Talus and Calcaneus (Part
of the Rearfoot Structures)
|
|
|
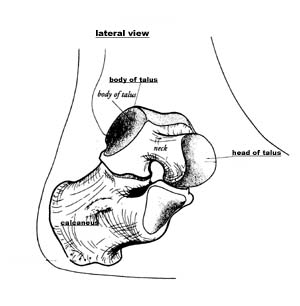
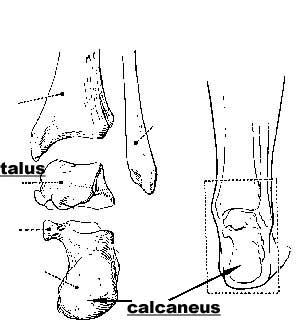
The talus and
the calcaneus are the two most posterior bones in the foot, as
well, as the largest of the tarsal bones of the foot. The talus
articulates with the distal tibia and fibula above to form the mortise
joint of the ankle. It articulates below with the calcaneus. No
muscles actually insert on the talus. The talus is moved indirectly
by muscles acting around it. (In the picture to the left the
talus is the bone on the top, and the calcaneus is the larger bone below
it) |
|
The superior aspect of the talus
is called the body. It has three articulating surfaces for articulation
with the tibia and fibula above. The head of the talus is located more
inferiorly and anteriorly and serves to articulates with the navicular
bones of the mid-foot and inferiorly to the calcaneus below. The
narrowed section between the body and the head is called the neck of the
talus. On the medially surface of the talus are two tubercles with a
groove between them. This groove is for the passage of the flexor
hallucis longus tendon. |
|
|
The calcaneus is
a large, irregularly-shaped bone. It
is a longer bone that comprises the rearmost portion of the foot that
strikes the ground at the heel. |
| The
posterior aspect of the calcaneus has a tuberosity for contact with the
ground at the heel. Near the middle of the bone, on its superior aspect,
is the articulation site with the talus above. The anterior projection
of the calcaneus has an articulation also with the talus, as well as
with the cuboid bone of the mid-foot. There is a prominent projection on
the medial portion of the calcaneus called the sustentaculum tali. This
projection has an accompanying groove through which tendons, and vessels
attach. On the posterior aspect of the calcaneus is an insertion area
for the large achilles tendon. |
|
| The
Midfoot Bony Structures |
|
|
Anterior
to the rearfoot complex of the calcaneus and talus is the midfoot.
It lies between the rearfoot, and the forefoot structures. If you view
the foot from the medial aspect and see the area commonly called the
“instep” this would correspond with the location of the midfoot
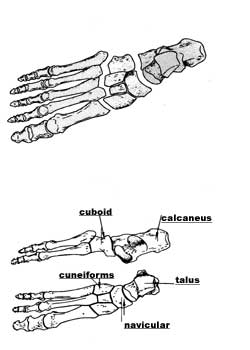
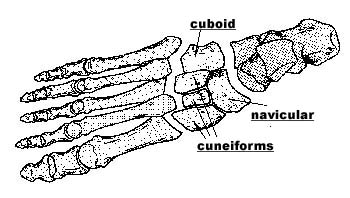
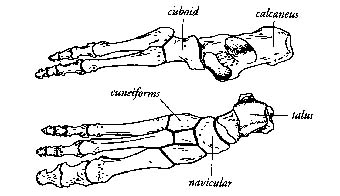
structures. There are five bones that make up the midfoot:
- the cuboid,
- the navicular,
- the 3 cuneiforms.
The navicular
articulates with the talus of the rearfoot on its proximal end.
The distal end of the navicular articulates with the 3 cuneiform bones.
It has a medial tubercle that can be felt externally on the foot. This
tubercle is for the insertion of the tibialis posterior muscle.
|
|
|
The cuboid
articulates proximally with the calcaneus of the rearfoot. It also
articulates with the navicular bone medially, and with the 3rd
cuneiform bone. It articulates with the metatarsals distally (forefoot
structures). A lateral bony notch is present that serves to hold the
tendon of the peroneus longus muscle.
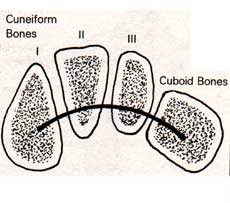
The
cuneiform bones are three small, edge-shaped bones with sharp
edges. They articulate with navicular proximally and with the
metatarsals distally. The mid-foot joints allow some degree of
flexibility in the foot.
(Notice
in the picture to the left the middle section, or midfoot, and how the
bony structures fit together. Note also which midfoot bones touch bones
in the other sections of the foot).
|
| The
Forefoot Bony Structures |
|

|
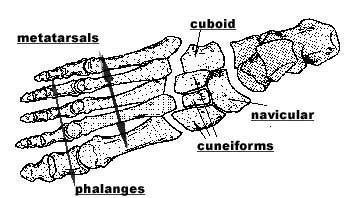
The most distal
aspect of the foot comprises the forefoot. It consists of two types of
bony structures:
- the metatarsals
- the phalanges
These bones are much like the bones of the
distal hand, except the big toe, unlike the thumb, is not opposable.
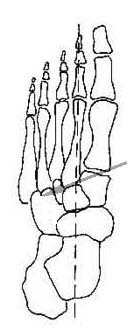
Each metatarsal consists of a
proximal base, a body, and a distal head. (See picture top left)
The base is mostly a square shape and has facets that articulate with
the tarsals of the mid-foot, as well as with adjacent metatarsals. The
head is round with a cartilaginous surface for articulation with the
proximal phalanx. The body is triangular like most long bones.
Each toe has a proximal, middle, and distal
phalanx as seem at left. The proximal phalanx is the longest. Collectively
they are called phalanges.
|
|
|
These all articulate
with each other to form the bony structure of the toes. |
|
|
| Lay-Out
of the Bones of the Foot |
|
|
| When all
of the bones of the foot are viewed together there are some important
anatomical combinations that are important functional units for the
foot. |
|

|
| Viewed
from the medial side of the foot you can see the longitudinal arch of
the foot. It runs front to back and forms the natural visible arch with
the floor or ground below.
The bones of the rearfoot, especially the
calcaneus forms the floor contact for the rear of the arch. The
metatarsal heads form the front contact point with the ground.
|
|
|
The foot is also
generally divided into the lateral foot and the
medial foot by joint articulations.
The lateral foot consists of:
- the calcaneus,
- the cuboid,
- and the metatarsals and phalanges of
toes 4 and 5.
It
includes the lateral arch of the foot and is more involved in weight
bearing activities during walking and running.
The medial foot consists of :
- the talus,
- the navicular,
- the cuneiforms,
- and the metatarsal and phalanges of toes
1, 2, and 3.
The medical foot includes the medial arch
and is more involved in propulsion (moving the body through space during
walking).
|
|
|
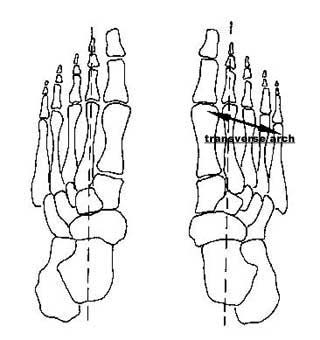
The bones of the
midfoot form the arch of the foot. Viewed from above the foot also has a
transverse arch that runs medial to lateral across the foot. The first
and fifth metatarsals are the contact points with the ground for this
arch. The bones of the mid-foot and the metatarsals form the elevated-
point for this arch.
Viewed from above the foot appears to
consist of 5 spokes (the metatarsals and toes) that splay out from the
tarsals behind them.
|
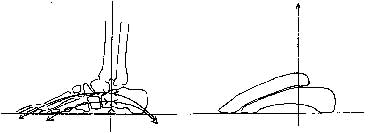
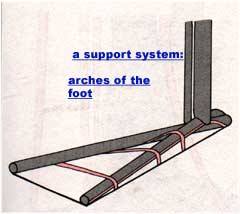
| In the
picture to the right you can see a schematic illustrating the support
system of the longitudinal and transverse arches of the foor. |
|
| Joints
of the Foot and Ankle
|
| The
joints in the foot and ankle are many and complex. In this course you
will be provided basic information about how these joints move, but the
actual biomechanics of the joints are quite complex, especially the sub-talar
joint.
|
| The
Ankle Joint |
|
|
The
ankle joint is comprised of the distal aspects of the tibia and
fibula that form a square shaped opening in which the body of the talus
fits. There are three articulations on the surface of the talus for
articulation with the tibia and fibula. Recall from the discussion above
that the body of the talus is dome shaped or rounded so that this
rounded surface fits into the opening above it. It is a snug fit for
this joint.
The
lateral malleolus extends down more distally along the lateral surface
of the talus. Because of this tight fit this joint is a pure hinge
joint – it only has available motion in one plane.
|
| The
ankle joint only moves in dorsiflexion and plantarflexion. It
does have a great deal of motion in both directions, more than any other
joints in the foot or ankle. When the foot moves into dorsiflexion the
body of the talus moves further into the joint space and makes the foot
tighter and more stable. When the foot moves into plantarflexion the
more narrow portion of the talus is in contact with the bones above and
thus the joint is less stable |
|
| The
Subtalar Joint |
|
|
Below the ankle
joint is the subtalar joint comprised of the articulations
between the talus and the calcaneus bones. There are two articulating
surfaces on each bone that form the joint. One surface is concave and
the other convex on each bone. In other words there is a dip and a bump
on each bone that fit into one another to form the joint. |
| The
calcaneus and the talus are not lined up equally and fit together so
that the talus is oriented more medially and the calcaneus more
laterally. Because this joint is biomechanically angular in its
orientation is has multiple planes in which movement occurs. The
subtalar joint produces plantarflexion and dorsiflexion, as well as
abduction and adduction of the foot. These two planar motions when
combined form the components of inversion and eversion of the ankle
which will be discussed more fully below.
|
| The
Transverse or Mid Tarsal Joints |
|
|
 © ©
|
Moving
distally along the ankle and foot, the next joints are the transverse
or mid tarsal joints. These are the joints between the rear foot and
the midfoot structures. There are two joints
- the talonavicular
- the calcaneocuboid.
The talus articulates with the
navicular bone to form the more medial talonavicular joint.The
calcaneus articulates with the cuboid to form the more lateral calcaneocuboid
joint.
Viewed
from above these joints are more of a curved shape across the middle of
the foot, rather than a straight line. Because of this shape is provides
motion of inversion and eversion of the foot. The transverse tarsal
joints have a key role in adjusting the foot when walking on uneven
surfaces.
|
| The
Cuneiform Joints |
|
| The
cuneiform bones articulate with the cuboid, the navicular, and each
other to make up the other portion of the midfoot joints. They also
participate in the inversion and eversion action at the midfoot.
|
|
|
 |
|
The Tarsometatarsal Joints |
|
|
Further distally
into the foot are the joint structures that split the midfoot from the
forefoot. The three cuneiform bones of the midfoot and the cuboid
articulate with the bases of the five metatarsal bones to form the tarsometatarsal
joints. |
|
|
The
joint line across the foot is irregular and does not form a straight
line. Metatarsal 1 articulates with the medial cuneiform. Metatarsal 2
fits into a notch formed by the three cuneiforms. Metatarsal 3
articulates with the most lateral cuneiform and Metatarsals 4 and 5 fit
against the cuboid bone. The available motions at these joints are
plantarflexion and dorsiflexion of
the midfoot. |
|
The Metatarsalphalangeal(MP) and
Interphalangeal(IP) Joints |
|
|
|
| The MP
and IP joints are the articulations of the heads of the metatarsals with
the proximal phalanges and the articulations of the proximal phalanges
to the middle phalanges, and the middle phalanges to the distal
phalanges. These are commonly referred to as the toe joints of the
foot. Toes
2-5 have three joints, and the great toe has only two since there is no
middle phalanx in the great toe. The great toe phalanges are much larger
than the phalanges bones of the other toes. It plays an important role
in walking when the toes are in contact with the ground.
The metatarsalphalangeal joints
allow three types of movement:
- dorsiflexion and plantar flexion of the
toes
- abduction and adduction of the toes
- slight medial lateral rotation.
The interphalangeal joints are
hinge joints that allow only plantarflexion and dorsiflexion of the
toes.
Plantarflexion of the toes has more
range of motion in the foot than Dorsiflexion. This allows the
individual to stand on tiptoe.
|
|
So
a quick recap of the joints:
- the
ankle joint is most proximal
- the
subtalar joint below it
- the
two midtarsal joints
- the
tarsometatarsal joints with the tarsals and the metatarsals of each
toe
- the
metatarsal joints with the proximal phalanges,
- the
joints of the phalanges that make up the distal toes.
The
ankle is a complex set of joints. Understanding the ligamentous support
is also important
|
| Ligaments
of the Foot and Ankle |
| There
are many small ligaments that connect the various bones of the foot and
ankle. There is also a larger ligamentous structure on the bottom of the
foot. These ligaments provide additional stability to the foot and
ankle. |
| The
Talofibular and Calcaneofibular Ligaments |
|
|
Thetalofibular and
calcaneofibular ligaments are probably the best known ligaments in the
body. This is the set of ligaments injured when someone rolls over on
the outside of the foot and sprains the ankle. The talofibular
ligaments are actually two small ligaments that run from the distal
end of the lateral malleolus of the fibula to the talus below. The calcaneofibular
ligament is a small ligament that runs from the distal malleolus of
the fibula to the calcaneus below. Together they form a 3 pronged
structure on the lateral (outside) aspect of the ankle.
These small ligaments can be easily
damaged or torn with spraining of the ankle. They help provide lateral
static stability to the ankle.
|
|
The Deltoid Ligament |
|

|
On the
medial aspect of the ankle is the deltoid ligament. It runs from
the medial malleolus of the tibia to the talus, and the navicular bone.
It is a broad, fan shaped ligament with two smaller ligaments beneath it
that provide a great deal of stability to the medial side of the ankle.
It is very unusual for someone to roll the ankle to the inside and
damage this ligament, rather a fracture of one of the bones would more
likely occur first. |
|
Other Smaller Ligaments in the Rearfoot and
the Midfoot |
| There
are several smaller ligaments that attach between the calcaneus, the
tibia, and the midtarsal bones. It is beyond the scope of this course to
discuss each ligament. It is important to remember, however, that the
presence of this network of ligaments between the bones of the foot
provide additional stability the foot requires for constant stresses of
weightbearing. |
|
| The
Plantar Ligament |
 |
| The
largest ligamentous structure in the foot is the plantar ligament.
It is also commonly called the plantar fascia. If you have heard someone
say that have plantar fascitis it is an inflammatory condition in this
ligament. The plantar ligament is on the bottom of the foot (the plantar
surface) and runs from the calcaneus to attach to the bases of
metatarsals II-V. It is quite a strong ligament and helps support the
arches of the foot. When seen on cadavers it appears thick and striated,
much like reinforced packing tape might be on a cardboard box. It is
impossible to tear that packing tape, it must be cut. The plantar fascia
is dense and strong to support the foot. |
|
Metatarsalphalangeal and Interphalangeal
Ligaments |
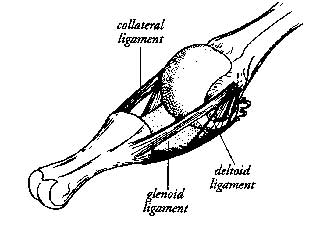 |
There are small
ligaments in the toes that have the same general arrangement. Each joint
has two collateral ligaments on each side of the joint.
There is a glenoid ligament on the bottom of the toe that runs
across the joint, and there is the deltoid or fanned shaped ligament
that runs from the proximal joint to the glenoid ligament border. These
ligaments provide stability at each of the small joints of the toe. |
| The
bones of the foot and ankle are many, but fit snugly together for
overall stability. The addition of several small ligaments attaching
bone-to-bone provides further stability. The large plantar ligament
provides a great deal of stability to the arch and bottom of the foot.
The final overlay of muscles then provides both dynamic and static
stability to the foot and ankle. The foot and ankle bear the brunt of
the weight of the body above it, as well as taking on the ground forces
beneath it. This will be discussed more fully later.
|
| Motions
of the Foot and Ankle |
|
|
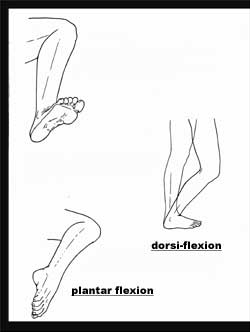
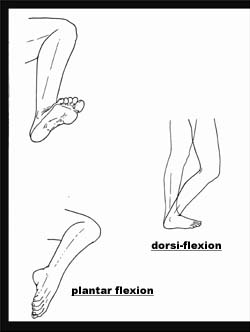
Dorsiflexion
– This motion is the pulling up of the foot. The toes are moving
closer to the front of the lower leg. The angle between the superior
surface of the foot and the anterior leg is getting smaller. In lay
language most people will say they “flex” the foot to achieve this
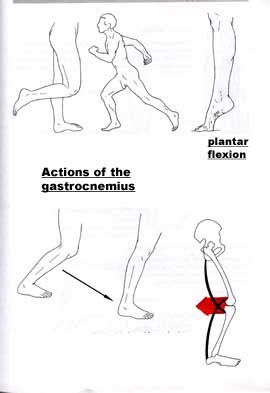
position. Dorsiflexion is
greater when the knee is flexed and less when the knee is extended. This
is because in knee extension there is greater tension on the
gastrocnemius muscles (the large muscle in the back of the lower leg). |
|

|
|
|

|
Plantarflexion
– This motion is moving the toes away from the front of the leg, or
increasing the angle between the superior surface of the foot and the
anterior leg. It is often referred to as extending the foot, or in dance
terms would be pointing the foot or toes. |
| Dorsiflexion
and Plantarflexion occur primarily at the ankle joint. You can also
dorsiflex or plantar flex the toes of the forefoot separate from the
rearfoot structures of the ankle. |
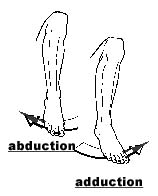
| Abduction –
This is moving the distal end of the foot away from midline, or away
from the center of the body. This motion occurs primarily at the
subtalar and more distal joints. |
|
Adduction –
This is moving the distal end of the foot toward the midline, or toward
the center of the body. This
motion occurs primarily at the subtalar and more distal joints. |
|
|
|
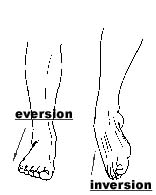
Inversion
– This is the combination movement of adduction and plantar
flexion at the ankle complex. When you perform this motion the sole
of the foot is directed toward the midline of the body with the great
toe pointing down slightly.
- Inversion = adduction +
plantarflexion
Eversion – This is the combination
movement of abduction and dorsiflexion at the ankle
complex. When you perform this motion the sole of the foot is directed
away from the midline of the body and the great toe is pointing up
slightly.
- Eversion = abduction + dorsiflexion
|
|
|
There is
more inversion at the ankle complex, than eversion due the biomechanical
arrangement of the bones. |
|
| Muscles
of the Foot and Ankle
|
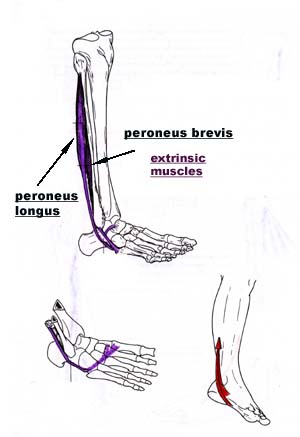
| Extrinsic
Versus Intrinsic Muscles
|
There
are two types of muscles in the foot and ankle:
- the extrinsic muscles
- the intrinsic muscles.
The extrinsic muscles originate on
the femur, tibia or fibula above and attach on the bones of the foot via
long tendons. All of these muscles cross more than one joint.
The intrinsic muscles of the foot
are short muscles that run between the smaller bones within the foot.
Most of these muscles are on the plantar surface (bottom) of the foot
and make up the bulk of the sole of the foot.
|
|
| Muscles
that Perform Dorsiflexion
|
There
are 4 primary dorsiflexors at the foot and ankle:
- the tibialis anterior
- the extensor hallucis longus
- the extensor digitorum longus
- the peroneus tertius.
These are all extrinsic muscles
located on the anterior aspect of the lower leg and ankle.
|
|
 |
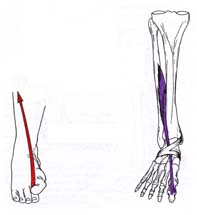
Tibialis
Anterior- This muscle originates from the lateral condyle and
superolateral shaft of the tibia and passes under the *extensor
retinaculum to insert on the medial cuneiform bone and the base of
the first metatarsal.
This muscle is the strongest dorsiflexor of
the foot and ankle. It also assists with inversion of the ankle. This
muscle passes down the front of the lower leg and attaches on the inside
(medial) aspect of the foot so when it contracts it pulls the foot up
and in.
*The extensor retinaculum is a thin sheath
of material that lies over the top of the foot to keep the long tendons
of the foot in place. It is visible in the picture to the left. You can
see the purple muscle passing under it as it proceeds onto the top of
the foot to attach on the base of the first metatarsal.
|
 |
Extensor
Hallucis Longus- This muscle
originates from the central anterior surface of the fibula and the
interosseus membrane and attaches to the base of the distal phalanx of
the great toe. It extends the great toe (pulls it up), but also assists
with dorsiflexion and inversion of the ankle. |
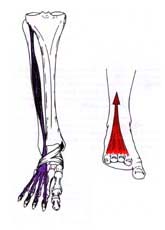 |
Extensor
Digitorum Longus- This muscle originates from the lateral tibial
condyle, the anterior fibular shaft, and the interosseus membrane. It
passes under the extensor retinaculum splits into four parts and
attaches to the bases of the distal phalanges of toes II-V. Its primary
function is to extend toes II-V (lift them up). It also performs
dorsiflexion of the ankle and eversion of the foot. |
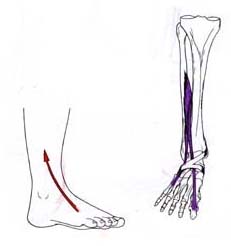 |
Peroneus
Tertius – This is a small muscle, absent in some people. It arises
from the anterior inferior portion of the fibula and attaches on the
fifth metatarsal. It performs dorsiflexion and eversion of the ankle.
In the picture to the left it is the
smaller, shorter muscle that attaches to the fifth metatarsal.
|
|
Muscles That Perform Plantarflexion |
There
are 7 muscles that perform plantarflexion at the foot and ankle:
- the gastrocnemius
- the soleus
- the peroneus longus
- the peroneus brevis
- the tibialis posterior
- the flexor hallucis longus and
- the flexor digitorum longus
|
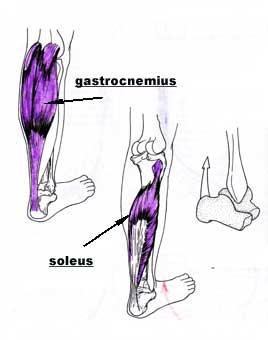
| Gastrocnemius
– This is a large, bulky muscle in the back of the lower leg and
functioning with soleus, are the primary plantar flexors of the ankle.
It arises from two heads on the distal posterior femur just above the
condyles. It inserts on the posterior/inferior surface of the calcaneus
via the Achilles tendon. The Achilles tendon is the strongest tendon in
the body, but is also often ruptured. The gastrocnenius performs
plantarflexion at the ankle. Because it also crosses the knee joint
above, it performs flexion and medial rotation of the knee. |
|
|
Soleus –
The soleus is a broader, deeper muscle located deep to the gastrocnemius,
but it does not cross the knee joint above. It arises from the
posterior/superior aspect of the tibia and fibula and merges with the
gastrocnemius to insert on the calcalneus via the Achilles tendon. Its
primary action is plantar flexion of the ankle especially during
walking. |
|
|
NOTE: Since
the gastrocnemius crosses the knee the position of the knee affects its
ability to plantar flex the ankle. When the knee is flexed the
gastrocnemius is on slack and is not an efficient plantar flexor of the
ankle. When the knee is extended the opposite is true.
To stretch the gastrocnemius you must put
stretch across both the ankle and the knee so the foot must be
dorsiflexed and the knee extended. To stretch the soleus the foot must
be dorsiflexed, but the knee must be flexed to eliminate the
gastrocnemius stretch.
Another important aspect of the
gastrocnemius occurs with weight bearing. When the leg is bearing weight
and the knee is flexed, the gastrocnenius works with the hamstring in
combination to become knee extensors.
|
|
|
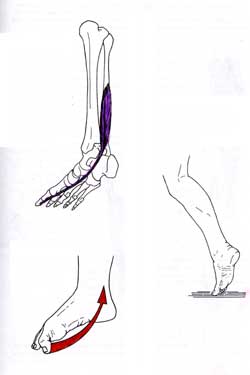
Peroneus Longus
– This muscle arises from the head and lateral/superior shaft of the
fibula. It follows a path down the lateral side of the leg passing
behind the lateral malleolus and goes under the lateral aspect of the
foot to attach on the plantar surface (bottom) of the foot on the medial
cuneiform and the base of the first metatarsal. It performs ankle
plantarflexion and eversion.
Peroneus Brevis – This muscle
arises from the shaft of the fibular, but more distally on the shaft
than peroneus longus. It also passes down the lateral aspect of the
lower leg and behind the lateral malleolus to insert on the lateral
tubercle of metatarsal V. Unlike peroneus longus, it does not go under
the foot. It also performs plantar flexion and eversion of the ankle.
|
|

|
Tibialis
Posterior – This is the deepest calf muscle. It originates from
the posterior/superior tibial and fibular shafts and the interosseus
membrane. It passes posterior to the medial malleolus on the inside of
the foot. It attaches primarily to the medial tubercle of the navicular
bone, with some smaller attachments to the cuboid, lateral cuneiform,
and metatarsal II-IV. It performs plantarflexion, and inversion of the
ankle. Since is passes under the medial side of the foot to attach on
the plantar surface it also serves to support the arch. |
| NOTE:
The combined attachments of Tibialis Posterior on the medial side of the
foot (inside) and the Peroneus Longus on the lateral side of the foot
(outside) work together to form a sling across the foot and support the
arch.
|
|
|
Flexor Hallucis
Longus – This muscle arises from
the posterior/inferior fibular and interosseus membrane and runs
posterior to the medial malleolus along a groove on the posterior talus,
passes to the underside of the foot to attach on the distal phalanx of
the great toe. It plantar flexes the great toe (pulls it under), plantar
flexes the ankle, and also supports the medial arch of the foot. |
|

|
Flexor
Digitorum Longus – This muscle originates from the
posterior/medial tibial shaft and runs posterior to the medial malleolus,
also goes to the underside of the foot and attaches on the distal
phalanges of toes II-V. Its action is plantar flexion of toes II-V
(pulls them under), and inversion of the foot. It also serves as an arch
support. |
|
|
As you
can see from the discussion of the muscles for dorsiflexion and plantar
flexion – these same muscles, depending on their location on the foot
serve as the muscles that perform inversion and eversion of the ankle as
well. Specifically, it splits as follows: |
| Muscles
Performing Inversion of the Ankle:
|
The
primary muscles that perform ankle inversion are:
- the tibialis anterior
- the tibialis posterior
- the extensor hallucis longus
- the flexor digitorum longus and
- the flexor hallucis longus.
These are all muscles that run from the
lower leg and attach on the medial aspect of the foot. When these
muscles contract they pull the insertion toward the origin and thus pull
the sole of the foot toward the inside or medial aspect of the body.
|
| Muscles
Performing Eversion of the Ankle:
|
The
primary muscles that perform ankle eversion are:
- the peroneus longus
- the peroneus brevis
- the peroneus tertius and
- the extensor digitorum.
These are all muscles that run from the
lower leg to attach on the lateral aspect of the foot. When these
muscles contract they pull the insertion of the muscles toward the
origin and thus pull the sole of the foot toward the lateral or outside
aspect of the body.
NOTE: You
will notice that the opposing actions of the foot and ankle are not
balanced. Plantar flexion has more muscles that perform this action, and
they are more powerful, than the muscles that perform Dorsiflexion.
Similarly, there are more muscles that perform Inversion than muscles
that perform Eversion at the ankle.
Plantarflexion and Inversion of the
ankle are stronger motions than Dorsiflexion and Eversion!
|
| Intrinsic
Muscles of the Foot
|
| These
are the smaller, shorter muscles that originate in the foot and attach
between the various bones in the foot. It is not within the scope of
this course to provide a great deal of detail on these muscles. They
will be discussed briefly. There is one intrinsic muscle that lies on
the dorsal (top) surface of the foot. The Extensor Digitorum Brevis
arises from the calcaneus and attaches on the phalanges of toes II-V. It
acts to dorsiflex the toes (pull them up in combination with the
extrinsic muscle the extensor digitorum longus already discussed. |
|
| The
opposite muscle on the plantar (bottom) surface of the foot is the Flexor
Digitorum Brevis. It arises from the inferior aspect of the
calcaneus and attaches on the middle phalanges II-V. It plantar flexes
the middle and proximal phalanges of toes II-V. Its action looks like a
“clawfoot” action of scrunching up the toes. |
| There
are similar intrinsic muscles on the dorsum and plantar surfaces of the
foot that flex the great
toe, abduct the great toe away from the other toes, move the great toe
toward the other toes, and abduct the 5th toe away from the
other toes. These muscles originates either on the calcaneus or on the
bones of the midfoot and attach on the metatarsals or phalanges of the
toes. These muscles include the Flexor Hallucis Brevis, Abductor
Hallucis, Adductor Hallucis, and Abductor Digiti Minimi. |
|
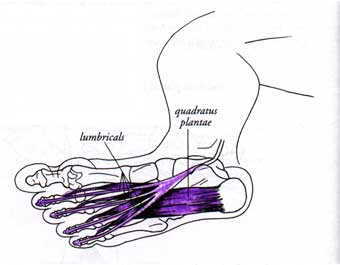
| The
other important intrinsic muscles of the foot are the Lumbricales
and the Interossei. |
|
|
| The Lumbricales
are four small muscles that run from the flexor digitorum longus
tendons up between the metatarsals inside the foot and
attach to the extensor digitorum longus tendons.
These muscles work to plantar flex the
middle phalangeal joints of the foot – to push the toes off the
ground during propulsion phase of walking.
|
| The Interossei
are the deepest layer of intrinsic muscles and occupy the space
between the metatarsals. There are 4 dorsal interossei more on the top
of the foot and 4 plantar interossei more on the bottom of the foot.
They act to plantar flex the proximal
phalanges which is also important during the propulsion phase of
walking.
|