Synopsis
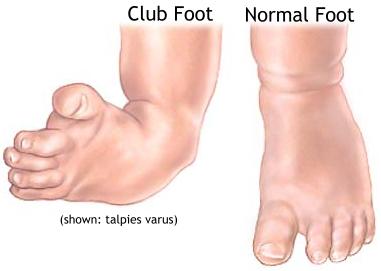
Clubfoot is a birth defect of unknown cause. True clubfoot is characterized by abnormal bone formation in the foot. There are four variations of clubfoot, known as talipes varus, talipes valgus, talipes equinus and talipes calcaneus. In talipes varus the foot generally turns inward so that the leg and foot look somewhat like the letter J. In talipes valgus the foot rotates outward like the letter L. In talipes equinus, the foot points downward, similar to a toe dancer. Finally, in talipes calcaneus, the foot points upward, with the heel pointing down. Talipes varus is the most common form of clubfoot.
Clubfoot is relatively common and
occurs more often in boys than in girls. It can affect one foot or both.
Sometimes a child's feet appear abnormal at birth because of the way the fetus
was positioned before birth. If there is no anatomic abnormality of the bone, it
is not true clubfoot and can usually be corrected by applying special braces or
casts to straighten the foot.
The cause of clubfoot is unclear, but is probably the result of several related factors, not one single cause. A combination of genetic and environmental factors, such as infections or drugs that may affect prenatal growth, seem to be responsible for the condition.
True clubfoot is usually obvious at birth. Uncorrected clubfoot in an adult causes only part of the foot, usually the outer edge, the heel, or the toes, to touch the ground. For a person with clubfoot, walking is difficult or impossible.
Diagnosis & TreatmentTrue clubfoot is usually obvious on physical examination. Diagnosis of clubfoot is confirmed by a routine x ray of the foot that shows the bones are malformed or misaligned. Ultrasonography does not always reveal the presence of club foot prior to the birth of the child.
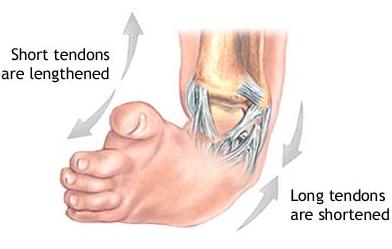
The sooner the treatment of clubfoot is started after birth the better, since an infant's foot contains large amounts of cartilage and the muscles, ligaments, and tendons are supple. In one common treatment, a series of casts is applied over a period of months to reposition the foot into a normal alignment. In mild cases, splinting and wearing braces at night may correct the deformity. In the most severe cases, surgery may be required, especially when the Achilles tendon needs to be lengthened. When clubfoot is severe enough to require surgery, the condition is usually not completely correctable, although significant improvement is possible. Long-term care by an orthopedist (a doctor who specializes in treatment of the skeletal system and its associated muscles and joints) is required after initial treatment to ensure that the correction of the deformity is maintained. Exercises, corrective shoes, or night-time splints may be needed until the child stops growing.
With prompt, expert treatment, clubfoot is usually correctable. Most individuals are able to wear regular shoes and lead active lives. If clubfoot is left untreated, the deformity becomes fixed, the growth of the leg and foot is affected, and some level of permanent disability results.
